Pediatric Epilepsy Syndromes 09
Topic: Pediatric
Created on Sunday, March 9 2008 by jdmiles
Last modified on Sunday, March 9 2008.
A) Psychiatry consultation for non-epileptic seizures
B) Prolonged video EEG
C) Repeat EEG in 2 months
D) Surgical resection of the seizure focus
E) Observation with follow-up
 | = Go back to the top of the page. |
 | = Reload a different version of this question (). |
 | = Load a random question from the database. |

| = Use this question as a template to create a totally NEW question. |
 | = Enter detailed rating for this question! |
 | = How users like you have rated this question. |
This question was last modified on March 09, 2008.
ANSWERS AND EXPLANATIONS
A) Psychiatry consultation for non-epileptic seizures
This answer is incorrect.
This child's history is very typical of Benign Childhood Epilepsy with Centrotemporal Spikes (also called BECTS, or "Benign Rolandic Epilepsy").
Children with this syndrome are otherwise normal neurologically, and typically remit spontaneously. Often, these seizures are not treated. If treated, seizures are usually responsive to monotherapy with most antiepileptic agents.
(See References) | | |
| | |
| Please log in if you want to rate questions. | |||||
B) Prolonged video EEG
This answer is incorrect.
This child's history is very typical of Benign Childhood Epilepsy with Centrotemporal Spikes (also called BECTS, or "Benign Rolandic Epilepsy").
Children with this syndrome are otherwise normal neurologically, and typically remit spontaneously. Often, these seizures are not treated. If treated, seizures are usually responsive to monotherapy with most antiepileptic agents.
Prolonged video EEG is unlikely to be of additional benefit in this patient.
(See References) | | |
| | |
| Please log in if you want to rate questions. | |||||
C) Repeat EEG in 2 months
This answer is incorrect.
This child's history is very typical of Benign Childhood Epilepsy with Centrotemporal Spikes (also called BECTS, or "Benign Rolandic Epilepsy").
Children with this syndrome are otherwise normal neurologically, and typically remit spontaneously. Often, these seizures are not treated. If treated, seizures are usually responsive to monotherapy with most antiepileptic agents.
The patient's current history and EEG are sufficient for this diagnosis. Repeating the EEG is unlikely to change this patient's management.
(See References) | | |
| | |
| Please log in if you want to rate questions. | |||||
D) Surgical resection of the seizure focus
This answer is incorrect.
This child's history is very typical of Benign Childhood Epilepsy with Centrotemporal Spikes (also called BECTS, or "Benign Rolandic Epilepsy").
Children with this syndrome are otherwise normal neurologically, and typically remit spontaneously. Often, these seizures are not treated. If treated, seizures are usually responsive to monotherapy with most antiepileptic agents.
(See References) | | |
| | |
| Please log in if you want to rate questions. | |||||
E) observation with follow-up
This answer is correct.
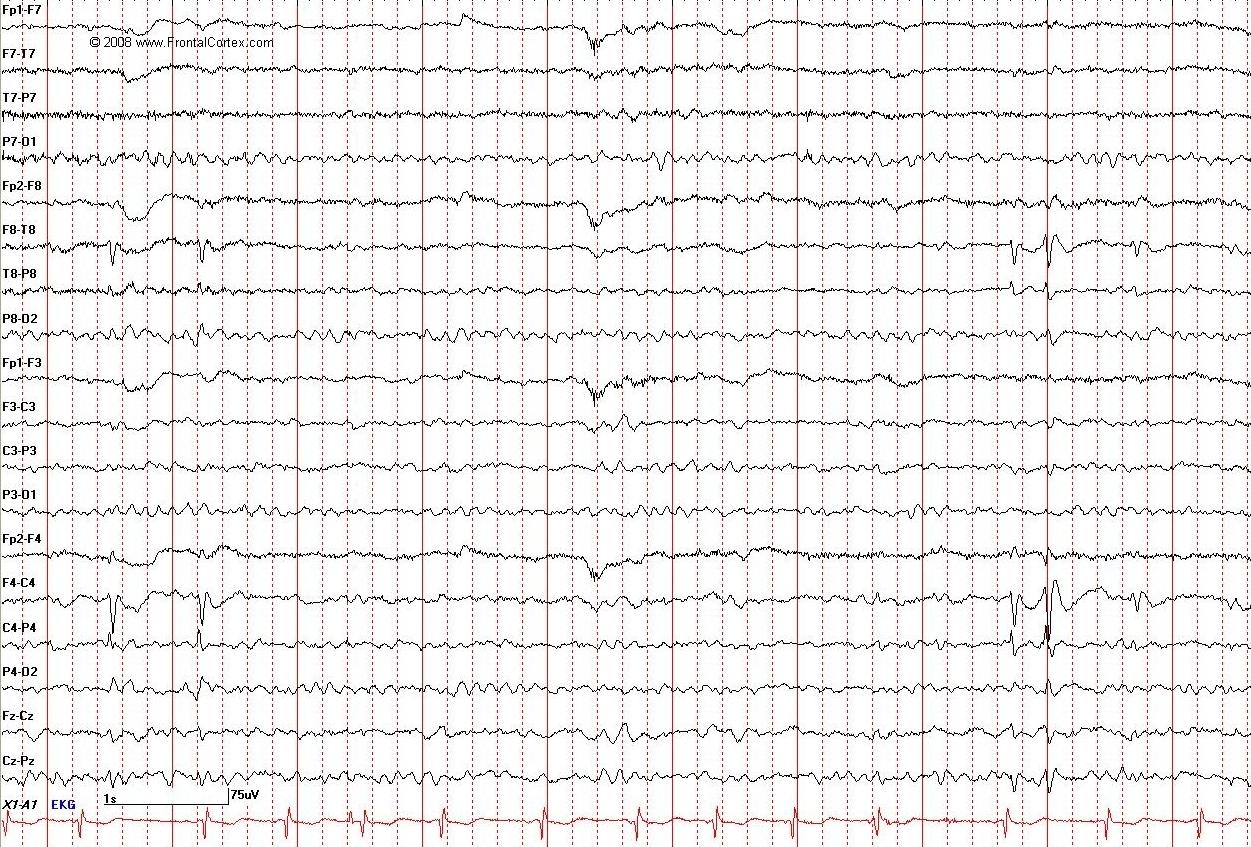
This child's history is very typical of Benign Childhood Epilepsy with Centrotemporal Spikes (also called BECTS, or "Benign Rolandic Epilepsy"), the most common focal childhood epilepsy syndrome. Onset of symptoms is between 4 and 12 years, most commonly at age 8 or 9. Seizure types are simple partial motor seizures involving the face, which usually occur during sleep or when the child wakes up. Children are usually brought to clinical attention after a generalized tonic clonic seizure, which represents the secondary generalization of one of these partial motor seizures. There is a family history of epilepsy in 40% of cases. This syndrome is strongly associated with EEG findings of centrotemporal sharp waves. These sharp waves have a maximal amplitude where the rolandic and sylvian fissures meet. Children with this syndrome are otherwise normal neurologically, and typically remit spontaneously. Often, these seizures are not treated. If treated, seizures are usually responsive to monotherapy with most antiepileptic agents. (See References)
| | |
| | |
| Please log in if you want to rate questions. | |||||
References:
| | |
| | |
| Please log in if you want to rate questions. | |||||
FrontalCortex.com -- Neurology Review Questions -- Neurology Boards -- Board Review -- Residency Inservice Training Exam -- RITE Exam Review
pediatric
Pediatric Epilepsy Syndromes 09
Question ID: 030908117
Question written by J. Douglas Miles, (C) 2006-2009, all rights reserved.
Created: 03/09/2008
Modified: 03/09/2008
Estimated Permutations: 7200
User Comments About This Question:
log in to FrontalCortex.com
New to FrontalCortex?
|

![]()
![]()

| | We comply with the HONcode standard for trustworthy health information: verify here. |
Share this page:
 |  |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
|
Friday, July 18, 2025 at 4:55:14 PM
This site has been visited 49961170 times since June 6 2006
All software and content (C) 2004-2025, FrontalCortex, Inc. unless otherwise specified.
privacy policy Web 2.0 policy disclaimer contact us
All software and content (C) 2004-2025, FrontalCortex, Inc. unless otherwise specified.
privacy policy Web 2.0 policy disclaimer contact us